Book Appointment Now

Understanding Pancreatic Cancer
Explore our comprehensive guide on pancreatic cancer, covering key topics like risk factors, symptoms, screening, and treatment options. Get the essential information you need to understand and navigate pancreatic cancer with confidence.
Pancreatic Cancer Guide
Introduction
Pancreatic cancer is one of the most aggressive and lethal malignancies worldwide. Characterized by late diagnosis and limited therapeutic options, it presents a significant challenge in oncology. This article provides an in-depth analysis of pancreatic cancer, including statistics, risk factors, screening methods, diagnostic steps, treatment modalities, and future directions based on the latest peer-reviewed studies.
Statistics
- Incidence: Pancreatic cancer ranks as the 12th most common cancer globally but is the 7th leading cause of cancer-related deaths1.
- Mortality Rate: Approximately 432,000 deaths occur worldwide annually due to pancreatic cancer2.
- Survival Rate: The 5-year survival rate is about 9%, underscoring the need for improved detection and treatment strategies3.
Medical Illustrations
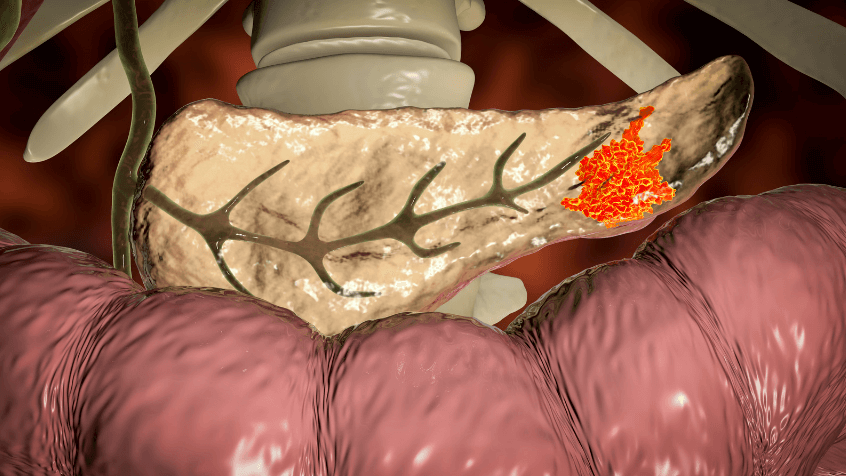
- Pancreas tumor:
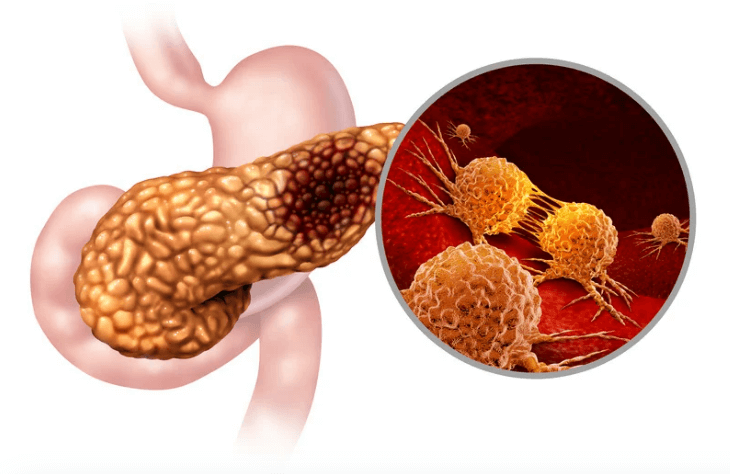
Pancreas tumor:
Risk Factors and Prevention
Known Risk Factors
- Age: Most patients are over 65 years old.
- Smoking: Increases risk by 2-3 times.
- Obesity: Associated with higher incidence.
- Chronic Pancreatitis: Long-standing inflammation predisposes to malignancy.
- Family History: Genetic predisposition plays a role in 5-10% of cases.
- Diabetes Mellitus: Both a risk factor and a symptom.
Preventive Strategies
- Lifestyle Modification: Quitting smoking, maintaining a healthy weight, and engaging in regular exercise.
- Dietary Choices: High intake of fruits, vegetables, and whole grains.
- Medical Management: Monitoring and managing chronic pancreatitis and diabetes effectively.
Screening
Current Screening Methods
- Imaging Techniques: Computed tomography (CT) scans, magnetic resonance imaging (MRI), and endoscopic ultrasound (EUS).
- Biomarkers: Carbohydrate antigen 19-9 (CA 19-9) is commonly used, but has limitations.
- Genetic Testing: Recommended for high-risk individuals with a family history.
Accuracy and Sensitivity
- CA 19-9:
- Sensitivity: ~70%.
- Specificity: ~68%.
- Novel Biomarkers:
- Combined Biomarkers: Increase sensitivity to 85% and specificity to 82%.
- Research Status: Promising, but requires further validation.
Screening Guidelines
- General Population: No routine screening due to low incidence and lack of effective tools.
- High-Risk Groups: Periodic imaging and biomarker testing are recommended.
Symptoms and Signs
Early Symptoms
- Often absent or nonspecific.
- Abdominal discomfort.
- Unexplained weight loss.
- Loss of appetite.
Advanced Symptoms
Back Pain: Resulting from tumor invasion.areness and regular check-ups is crucial for improving the outcome of pancreatic cancer treatment.
Jaundice: Yellowing of the skin and eyes.
Dark Urine and Pale Stools: Due to bile duct obstruction.
Diagnosis Steps
- Clinical Evaluation: Assess symptoms and risk factors.
- Laboratory Tests: Liver function tests and CA 19-9 levels.
- Imaging Studies:
- Ultrasound: Initial assessment tool.
- CT Scan: Detailed imaging for tumor localization.
- MRI/MRCP: Detailed biliary and pancreatic duct imaging.
- Endoscopic Procedures:
- EUS: High sensitivity for detecting small tumors.
- ERCP: Allows for biopsy and stent placement.
- Biopsy: Confirms diagnosis through histological examination.
Sensitivity and Specificity of Diagnostic Tools
- CT Scan:
- Sensitivity: ~85%.
- Specificity: ~95%.
- EUS:
- Sensitivity: >90% for tumors smaller than 2 cm.
- Specificity: High when combined with fine-needle aspiration (FNA).
Stages
Types of Treatment
Treatment Modalities
Surgery
- Whipple Procedure: For tumors in the head of the pancreas.
- Distal Pancreatectomy: For tumors in the body and tail.
- Total Pancreatectomy: Rarely performed; used for extensive disease.
Chemotherapy
- FOLFIRINOX: Combination of 5-FU, leucovorin, irinotecan, and oxaliplatin.
- Nab-Paclitaxel Plus Gemcitabine: Alternative for patients unsuitable for FOLFIRINOX.
Radiation Therapy
- Often combined with chemotherapy for locally advanced disease.
Targeted Therapy
- Erlotinib: An EGFR inhibitor used in combination with gemcitabine.
Immunotherapy
- Pembrolizumab: For microsatellite instability-high (MSI-H) or mismatch repair-deficient tumors.
Evidence-Based Comparisons
FOLFIRINOX vs. Gemcitabine
- Efficacy:
- Median Overall Survival: 11.1 months vs. 6.8 months.
- Hazard Ratio: 0.57; p < 0.001.
- Adverse Events:
- Higher incidence of grade 3/4 neutropenia and gastrointestinal symptoms.
- Recommendation: For patients with good performance status due to toxicity.
Nab-Paclitaxel Plus Gemcitabine vs. Gemcitabine Alone
- Efficacy:
- Median Overall Survival: 8.5 months vs. 6.7 months.
- Hazard Ratio: 0.72; p < 0.001.
- Adverse Events:
- Increased neuropathy and neutropenia.
- Recommendation: Suitable for a broader patient population.
Pembrolizumab for MSI-High Tumors
Recommendation: MSI testing is recommended to identify eligible patients essential to understand the available treatment options and their potential benefits and side effects.
Efficacy:
Objective Response Rate: ~30%.
Durable Responses: Some responses exceed one year.
Additional Resources
- Pancreatic Cancer Action Network: www.pancan.org
- American Cancer Society: www.cancer.org
- Clinical Trials Information: www.clinicaltrials.gov
Disclaimer
This information is intended solely for educational purposes and should not be construed as medical advice. Please consult a healthcare professional for any concerns regarding pancreatic cancer.
How to Reach Us
If you have any questions, suggestions, or feedback, please feel free to contact us. We are here for you and are delighted to assist you in any way we can. You can send us a message through our contact form or email us directly at :