Book Appointment Now

Understanding Liver Cancer
Explore our comprehensive guide on liver cancer, covering key topics like risk factors, symptoms, screening, and treatment options. Get the essential information you need to understand and navigate liver cancer with confidence.
Liver Cancer Guide
Introduction
Liver cancer, primarily hepatocellular carcinoma (HCC), is a malignancy originating from hepatocytes, the main functional cells of the liver. Historically, liver cancer has been closely associated with chronic viral hepatitis infections and alcohol-induced liver disease. In recent years, non-alcoholic fatty liver disease (NAFLD) has emerged as a significant risk factor due to the global rise in obesity and diabetes. Recent developments in systemic therapies, including targeted agents and immunotherapies, have begun to improve outcomes for patients with advanced disease. Studying liver cancer is crucial because of its increasing incidence, high mortality rate, and the potential for prevention through vaccination and lifestyle modifications.
Statistics
Statistical Overview
Liver cancer is a major global health challenge. According to the World Health Organization (WHO) in 2020:
- Incidence: Approximately 905,000 new cases worldwide.
- Mortality: Around 830,000 deaths, making it the third leading cause of cancer-related deaths globally.
Key Disparities
- Gender:
- Men: Historically higher incidence and mortality rates, though rates are decreasing due to reduced smoking.
- Women: Incidence rates are stabilizing or increasing in some regions, reflecting past smoking trends.
- Age:
- Most cases occur in individuals over 50 years.
- Younger patients may be affected in regions with high hepatitis B virus (HBV) prevalence.
- Geography:
- High Incidence Regions:
- East Asia (e.g., China, Mongolia)
- Sub Saharan Africa (e.g., Gambia, Mali)
- Lower Incidence Regions:
- North America
- Europe
- Note: Incidence is rising in low-incidence regions due to NAFLD and hepatitis C virus (HCV) infections.
- High Incidence Regions:
Key Statistics
- 5-Year Survival Rates:
- Localized Disease: Approximately 31%.
- Regional Spread: About 11%.
- Distant Metastasis: Around 3%.
- Overall: Approximately 20%, reflecting late-stage diagnoses and limited treatment options.
- Trends Over Time:
- Increasing Incidence: Global rates have more than doubled since the 1990s.
- Mortality Rates: Have risen parallel to incidence, indicating the aggressive nature of the disease.
Global maps present (A) 20 areas of the world and (B) the four-tier Human Development Index.
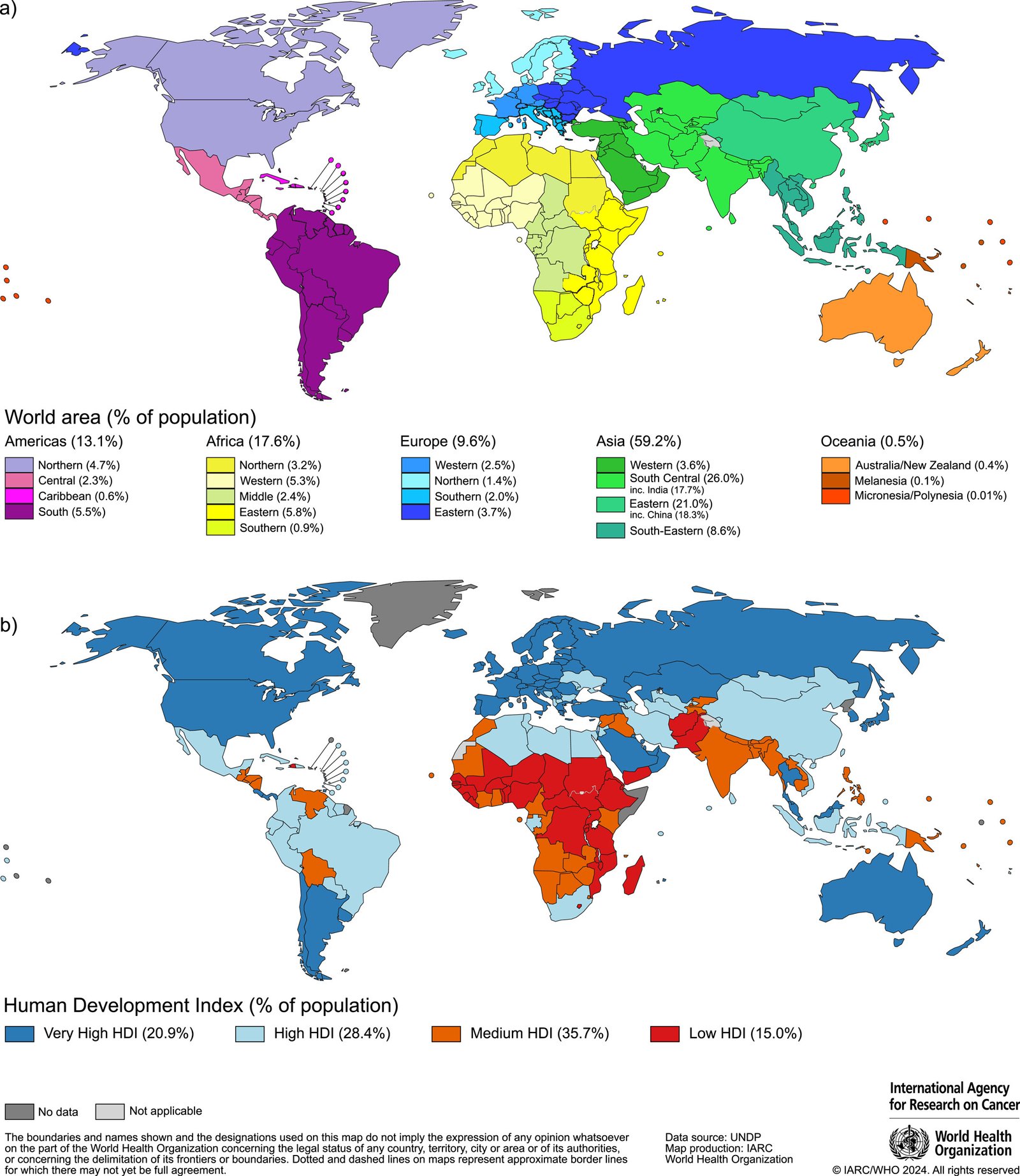
Source: International Agency for Research on Cancer (IARC)
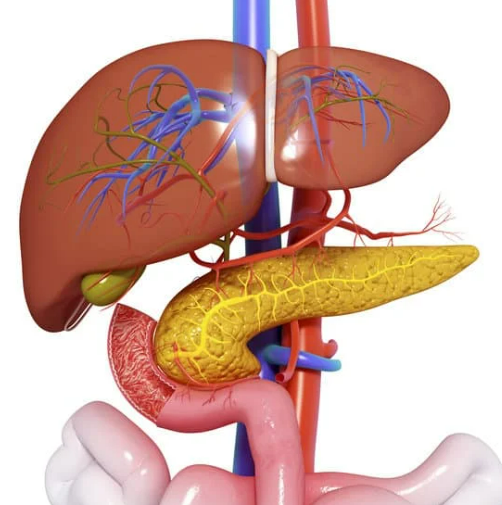
Medical Illustrations
Liver cancer:
Image soorces: https://www.mayoclinic.org/

Hepatocellular Carcinoma:
Image courtesy of Arief Suriawinata, MD, Department of Pathology, Dartmouth Medical School.

Risk Factors and Prevention
a. Known Risk Factors
Environmental Factors:
- Chronic Viral Hepatitis:
- Hepatitis B Virus (HBV):
- Leading cause globally, especially in Asia and Africa.
- Mechanism: Chronic infection leads to inflammation, fibrosis, and genetic mutations.
- Hepatitis C Virus (HCV):
- Significant cause in Western countries.
- Mechanism: Similar to HBV, causing chronic liver damage.
- Hepatitis B Virus (HBV):
- Alcohol Consumption:
- Heavy Drinking:
- Leads to alcoholic liver disease, cirrhosis, and increased cancer risk.
- Threshold: Consumption exceeding 80 grams/day for men, 40 grams/day for women.
- Heavy Drinking:
- Non-Alcoholic Fatty Liver Disease (NAFLD):
- Associated Conditions:
- Obesity, type 2 diabetes, metabolic syndrome.
- Progression: Can lead to non-alcoholic steatohepatitis (NASH), fibrosis, and HCC.
- Associated Conditions:
- Exposure to Aflatoxins:
- Sources:
- Contaminated grains and nuts in developing countries.
- Effect: Potent carcinogens causing genetic mutations.
- Sources:
Genetic Factors:
- Hereditary Hemochromatosis:
- Iron overload disorder increases HCC risk.
- Mechanism: Excess iron leads to oxidative stress and DNA damage.
- Alpha-1 Antitrypsin Deficiency:
- Causes liver accumulation of abnormal proteins, leading to cirrhosis and cancer.
Recent Studies:
- A meta-analysis in The Lancet Gastroenterology & Hepatology (2021) confirmed the rising incidence of NAFLD-related HCC.
- Research in Hepatology (2022) linked genetic polymorphisms in PNPLA3 to increased HCC risk in NAFLD patients.
b. Preventive Strategies
Vaccination:
- Hepatitis B Vaccination:
- Effectiveness: Reduces HBV infection rates and subsequent HCC development.
- Implementation: WHO recommends universal infant vaccination.
Antiviral Therapies:
- HBV and HCV Treatments:
- Nucleos(t)ide Analogues (e.g., entecavir, tenofovir) for HBV suppress viral replication.
- Direct-Acting Antivirals (DAAs) for HCV achieve sustained virologic response (SVR).
- Evidence: SVR reduces HCC risk by up to 75% (Study: Annals of Internal Medicine, 2019).
Lifestyle Modifications:
- Alcohol Reduction:
- Limiting intake reduces progression to cirrhosis and HCC.
- Weight Management:
- Diet and exercise to prevent NAFLD and NASH.
- Diabetes Control:
- Tight glycemic control may reduce HCC risk.
Chemoprevention:
- Use of Statins:
- Some studies suggest statins may lower HCC risk, especially in HBV-infected individuals.
- Coffee Consumption:
- Meta-analyses indicate an inverse relationship between coffee intake and HCC risk.
Public Health Measures:
- Aflatoxin Control:
- Proper food storage to prevent contamination.
- Safe Injection Practices:
- Reducing HBV and HCV transmission.
Screening
Current Screening Methods
Ultrasound (US):
- Efficacy:
- Sensitivity: Approximately 60-80% for detecting early-stage HCC.
- Specificity: Around 90%, meaning few false positives.
- Frequency:
- Every 6 months for high-risk individuals (e.g., cirrhosis patients).
- Advantages:
- Non-invasive, widely available, cost-effective.
- Limitations:
- Operator-dependent, less effective in obese patients.
Alpha-Fetoprotein (AFP) Testing:
- Efficacy:
- Sensitivity: Low when used alone (~40-60%).
- Specificity: Improved when combined with US.
- Usage:
- Often used alongside US to increase detection rates.
- Limitations:
- Elevated AFP can occur in other liver diseases.
Advanced Imaging:
- Contrast-Enhanced MRI or CT:
- Used for diagnostic confirmation, not routine screening.
- Advantages:
- Higher sensitivity and specificity.
- Limitations:
- Costly, not practical for regular screening.
Comparative Summary:
- Ultrasound with or without AFP is the standard screening method for high-risk populations due to its balance of effectiveness and practicality.
Symptoms and Signs
Early-Stage Symptoms:
- Often asymptomatic; highlights the importance of regular screening in high-risk groups.
Intermediate-Stage Symptoms:
- Upper Abdominal Pain:
- Dull ache or fullness in the right upper quadrant.
- Weight Loss:
- Unintentional and significant.
- Fatigue:
- Generalized weakness.
- Jaundice:
- Yellowing of skin and eyes due to bile duct obstruction.
Advanced-Stage Symptoms:
- Ascites:
- Accumulation of fluid in the abdomen.
- Encephalopathy:
- Confusion due to liver dysfunction.
- Gastrointestinal Bleeding:
- From esophageal varices due to portal hypertension.
Misdiagnoses and Atypical Presentations:
- Case Anecdote:
- A 55-year-old patient with a history of heavy alcohol use presented with vague abdominal discomfort, initially treated for gastritis. Further investigation revealed advanced HCC.
- Challenges:
- Symptoms often overlap with other liver diseases, delaying diagnosis.
Diagnosis Steps
- Initial Assessment:
- Medical History:
- Evaluate risk factors: HBV/HCV status, alcohol use, family history.
- Physical Examination:
- Look for signs of chronic liver disease: jaundice, ascites, hepatomegaly.
- Medical History:
- Laboratory Tests:
- Liver Function Tests (LFTs):
- Assess levels of ALT, AST, ALP, bilirubin.
- AFP Level:
- Elevated in many HCC cases.
- HBV and HCV Serology:
- Determine viral infection status.
- Liver Function Tests (LFTs):
- Imaging Studies:
- Ultrasound:
- Initial imaging modality to detect masses.
- Contrast-Enhanced MRI or CT Scan:
- Triple-Phase Imaging:
- Arterial, portal venous, and delayed phases to characterize lesions.
- Triple-Phase Imaging:
- Gadoxetic Acid-Enhanced MRI:
- Improves detection of small lesions.
- Ultrasound:
- Biopsy Procedures:
- Percutaneous Liver Biopsy:
- Obtains tissue for histological confirmation.
- Risks:
- Bleeding, tumor seeding; often avoided if imaging is characteristic.
- Percutaneous Liver Biopsy:
- Non-Invasive Techniques:
- Liquid Biopsy:
- Emerging method analyzing circulating tumor DNA.
- Liquid Biopsy:
- Tumor Marker Analysis:
- AFP-L3:
- A specific isoform linked to HCC.
- Des-Gamma-Carboxy Prothrombin (DCP):
- Another marker aiding diagnosis.
- AFP-L3:
- Staging:
- Barcelona Clinic Liver Cancer (BCLC) Staging System:
- Considers tumor size, liver function, performance status.
- TNM Classification:
- Tumor size, lymph node involvement, metastasis.
- Barcelona Clinic Liver Cancer (BCLC) Staging System:
Stages
Types of Treatment
Treatment Modalities
Surgical Resection:
- Indications:
- Early-stage HCC with preserved liver function (Child-Pugh A).
- Outcomes:
- 5-year survival rates of 50-70%.
- Side Effects:
- Bleeding, infection, liver failure.
Liver Transplantation:
- Indications:
- Early-stage HCC within Milan criteria (single tumor ≤5 cm or up to 3 tumors ≤3 cm).
- Outcomes:
- 5-year survival rates over 70%.
- Side Effects:
- Rejection, immunosuppression complications.
Locoregional Therapies:
- Radiofrequency Ablation (RFA):
- Mechanism: Destroys tumors with heat.
- Indications: Tumors ≤3 cm.
- Side Effects: Pain, risk of bleeding.
- Transarterial Chemoembolization (TACE):
- Mechanism: Delivers chemotherapy directly to the tumor while blocking blood supply.
- Indications: Intermediate-stage HCC not amenable to surgery.
- Side Effects: Post-embolization syndrome (fever, pain), liver dysfunction.
Systemic Therapies:
- Targeted Therapies:
- Sorafenib:
- Mechanism: Multikinase inhibitor targeting tumor proliferation and angiogenesis.
- Side Effects: Hand-foot skin reaction, diarrhea, hypertension.
- Efficacy: Median OS improvement of ~3 months.
- Lenvatinib:
- Mechanism: Inhibits VEGFR, FGFR, PDGFR.
- Side Effects: Hypertension, fatigue, decreased appetite.
- Efficacy: Non-inferior to sorafenib with median OS of 13.6 months.
- Sorafenib:
- Immunotherapy:
- Nivolumab:
- Mechanism: PD-1 inhibitor enhancing immune response.
- Side Effects: Immune-related adverse events (colitis, hepatitis).
- Efficacy: ORR of 14%, durable responses.
- Atezolizumab plus Bevacizumab:
- Mechanism: Combines PD-L1 inhibition with anti-angiogenesis.
- Side Effects: Hypertension, proteinuria, bleeding risk.
- Efficacy: Median OS of 19.2 months, superior to sorafenib.
- Nivolumab:
Evidence-Based Comparisons
| Treatment | Mechanism | Side Effects | Efficacy (Survival Rate) | Study/Trial |
|---|---|---|---|---|
| Sorafenib | Multikinase inhibitor (VEGFR, RAF) | Hand-foot skin reaction, diarrhea | Median OS ~10.7 months | SHARP Trial, 2008 |
| Lenvatinib | Inhibits VEGFR, FGFR, PDGFR | Hypertension, fatigue | Median OS ~13.6 months | REFLECT Trial, 2018 |
| Atezolizumab + Bevacizumab | PD-L1 inhibitor + VEGF inhibitor | Hypertension, proteinuria, bleeding | Median OS ~19.2 months | IMbrave150 Trial, 2020 |
| Nivolumab | PD-1 inhibitor | Immune-mediated reactions | ORR ~14%; median OS not reached | CheckMate 040, 2017 |
Key Studies:
- SHARP Trial (2008):
- Findings: Sorafenib improved median OS by nearly 3 months over placebo.
- Clinical Significance: First systemic therapy approved for advanced HCC.
- REFLECT Trial (2018):
- Findings: Lenvatinib was non-inferior to Sorafenib with better PFS and ORR.
- Clinical Significance: Provides an alternative first-line treatment.
- IMbrave150 Trial (2020):
- Findings: Atezolizumab plus Bevacizumab significantly improved OS and PFS compared to Sorafenib.
- Clinical Significance: Established a new standard of care for first-line therapy.
Additional Resources
- Patient Advocacy Groups:
- Key Opinion Leaders:
- Dr. Ghassan Abou-Alfa: Expert in liver cancer clinical trials.
- Dr. Ann-Lii Cheng: Leading researcher in targeted therapies.
- Clinical Trials:
- ClinicalTrials.gov: Comprehensive database of ongoing liver cancer studies.
- National Cancer Institute Trials
Key Findings
- Liver Cancer Incidence is Increasing Globally: Driven by viral hepatitis, NAFLD, and alcohol use.
- Early Detection Enhances Survival: Regular screening in high-risk populations is crucial.
- Advancements in Systemic Therapies: New treatments like Atezolizumab plus Bevacizumab have improved survival rates.
- Prevention is Effective: HBV vaccination and antiviral treatments reduce liver cancer risk.
- Lifestyle Factors are Modifiable Risks: Addressing obesity, alcohol consumption, and diabetes can lower incidence.
Discussion
The rising incidence and mortality of liver cancer globally highlight the urgent need for effective prevention, early detection, and treatment strategies. While HBV and HCV infections remain significant risk factors, the growing impact of NAFLD due to lifestyle changes underscores the importance of public health interventions.
Screening programs using ultrasound, with or without AFP testing, have been shown to improve early detection rates, yet their implementation varies worldwide. Advances in imaging and the development of biomarkers hold promise for enhancing screening efficacy.
Treatment options have expanded with the advent of targeted therapies and immunotherapies, leading to improved survival outcomes. However, challenges remain in determining the optimal sequencing of treatments and managing resistance mechanisms.
Discrepancies in access to care, particularly in low-income regions with the highest burden of disease, contribute to global survival disparities. Addressing these inequities is essential for improving overall outcomes.
Final Recommendations
Clinical Recommendations:
- Implement Regular Screening:
- Ultrasound every 6 months for high-risk individuals (e.g., cirrhosis patients).
- Adopt New Treatment Protocols:
- Incorporate Atezolizumab plus Bevacizumab as first-line therapy where available.
- Promote Multidisciplinary Care:
- Collaboration among specialists to optimize patient outcomes.
Research Directions:
- Develop Sensitive Biomarkers:
- Focus on identifying markers for early detection and treatment response.
- Investigate Combination Therapies:
- Explore synergistic effects of targeted agents and immunotherapies.
- Understand Resistance Mechanisms:
- Research to overcome therapeutic resistance and improve efficacy.
Policy Suggestions:
- Enhance Vaccination Programs:
- Ensure universal HBV vaccination and access to antiviral therapies.
- Address Lifestyle Factors:
- Implement public health campaigns targeting obesity, alcohol use, and diabetes management.
- Improve Access to Care:
- Increase availability of screening and advanced treatments in underserved regions.
Disclaimer
The information provided in this article is intended for general informational purposes only and should not be construed as medical advice. While every effort has been made to ensure the accuracy of the information presented, it is not a substitute for professional medical guidance, diagnosis, or treatment. Always consult a qualified healthcare provider with any questions you may have regarding a medical condition, including liver cancer. Do not disregard or delay seeking professional medical advice based on information found in this article. The authors and publishers are not responsible for any consequences resulting from the use of the information provided.
How to Reach Us
If you have any questions, suggestions, or feedback, please feel free to contact us. We are here for you and are delighted to assist you in any way we can. You can send us a message through our contact form or email us directly at :